

Joseph R. Anticaglia MD
Medical Advisory Board
Parkinson’s disease (PD) is an adult onset, progressive, nerve wasting, movement disorder of the brain causing a depletion of the hormone dopamine. PD attacks a part of the brain called the substantia nigra, which produces dopamine. This chemical messenger in the brain, dopamine, plays a key role in muscle tone and movement. Treatment is primarily focused on replenishing the brain with dopamine.
About a million Americans have PD, men more than women, and about 60,000 people in the U. S. each year are diagnosed with this disease. Although there are significant non-movement symptoms associated with Parkinson’s, treatment is particularly directed at relieving movement—motor symptoms, such as:
- Tremor — shakiness
- Balance instability
- Bradykinesia — slowing of automatic and spontaneous movement
- Rigidity — muscle stiffness
- Walking/gait problems — freezing
Because PD patients are dopamine deficient, prescribing drugs that enhance dopamine is the key element in the treatment of this disease.

Non-Medical Treatments
Exercise is useful for physical, emotional, and mental health. It’s an important partner in the management of Parkinson’s disease. Besides aerobic, strength and flexibility exercises balance exercises have been shown to improve gait, stability, and motor coordination in PD patients. It provokes neurons to produce dopamine. Furthermore, it combats fatigue and depression. Exercise such as a stationary bike, using the treadmill, yoga, and Tai Chi have proven to be beneficial.
Diet — Nutrition
Enjoy a healthy diet with a variety of foods, low in saturated fats and with a moderate amount of salt and sugars. Increase fiber and fluids in the diet. PD patients are at risk for weight loss and malnutrition because of difficulty they have chewing and swallowing. Increase healthy foods that are soft and easy to swallow in their diet. Avoid taking the PD medication Sinemet (see below) with foods high in protein such as beans, dairy, eggs or meats. They interfere with the absorption of this medication.
Speech — Balance
Consider consulting a Speech Pathologist for patients with slurred speech or low volume speech. Also, consider the assistance of a Physical Therapist, for instance, to improve balance and stability, to increase muscle strength and to reduce muscle and joint stiffness.
Psychosocial Issues
PD patients may experience anxiety, depression, and fear. A sense of isolation and lack of enthusiasm reinforce the misguided notion that PD symptoms are limited to what we see. Professional counseling is advised in these situations. Seek out local, PD, support groups.
Medical Treatments
A deficiency of dopamine was first identified in PD patients in the 1960s. Oral levodopa was introduced as the treatment for Parkinson’s in 1967, and it has remained the “gold standard” in the management of people with this disease.
Parkinson’s treatment depends on the patient’s symptoms. Dopaminergic drugs mimic dopamine and temporarily replenish the lack of dopamine. They don’t cure PD and do not slow the progression of this disease. If Parkinson’s disease does not interfere with the quality of a person’s life, it’s best not to start drug treatment.
The release of sufficient amounts of dopamine in the midbrain allows individuals to have controllable, coordinated muscle movement. When there is an inadequate amount of this drug, PD patients experience involuntary movements, poor balance, shakiness, muscle stiffness and other symptoms. Dopamine, in combination with other medications, has restored smooth and organized muscle movement to these individuals.
Carbidopa-Levodopa (Sinemet)
Dopamine is incapable of crossing the blood-brain barrier and entering the brain. In addition.
the medication Levodopa cannot enter the brain on its own. However, the combination of carbidopa-levodopa allows levodopa to enter the brain; and once inside the brain, levodopa turns into dopamine. Also, carbidopa prevents the breakdown of levodopa in the bloodstream, and diminishes or prevents some of the side effects of levodopa such as nausea and vomiting.
As the disease progresses, one drawback of long-term use of levodopa is dyskinesia — the development of involuntary movements (e. g., Michael Fox). Also, the beneficial effects of levodopa become less consistent with years of use in this progression disease. The medication is still working but requires upward dosage adjustment. For these reasons, specialists recommend starting the treatment of PD with a class of drugs called dopamine agonists.
Dopamine agonists are medications that imitate dopamine and stimulate dopamine receptors in the brain to produce dopamine. Examples in this class of drugs are pramipexole (Mirapex) and ropinirole (Requip). If the symptoms of the PD are not controlled by agonists, consideration
is given to using it along with levodopa to treat the patient’s symptoms. Worrisome, side effects due to this drug include compulsive gambling and shopping, binge eating, and hypersexuality.
COMT inhibitors are drugs that work only when used with carbidopa-levodopa. They block the enzyme that breaks down levodopa and dopamine. As a result, they prevent the “wearing off” of the drug before the next dose.
Anticholinergic drugs are used to help control tremors and muscle rigidity. They are prescribed cautiously to elderly patients because of the unwanted effects of worsening cognition and constipation.
Amantadine is an antiviral agent that can provide relief of PD in its early stage with mild symptoms but no disability. It may also be used to control dyskinesia caused by carbidopa-levodopa. MAO-B inhibitors block the breakdown of dopamine and may improve the fluctuation or declining effect of levodopa.
Side Effects of Medications
Parkinson’s patients need to be aware of what medications they are taking and for what purpose. Some of the unwanted effects of taking PD medication have been noted above; for example, dyskinesia. The side effects of Sinemet include dizziness, nausea, and vomiting. The drug compazine (prochlorperazine), given for nausea and vomiting, can cause symptoms that mimic motor PD. Patients taking dopamine agonists’ have experienced hallucination and delusions. Delusions and hallucinations may occur as the disease progresses.
Surgery
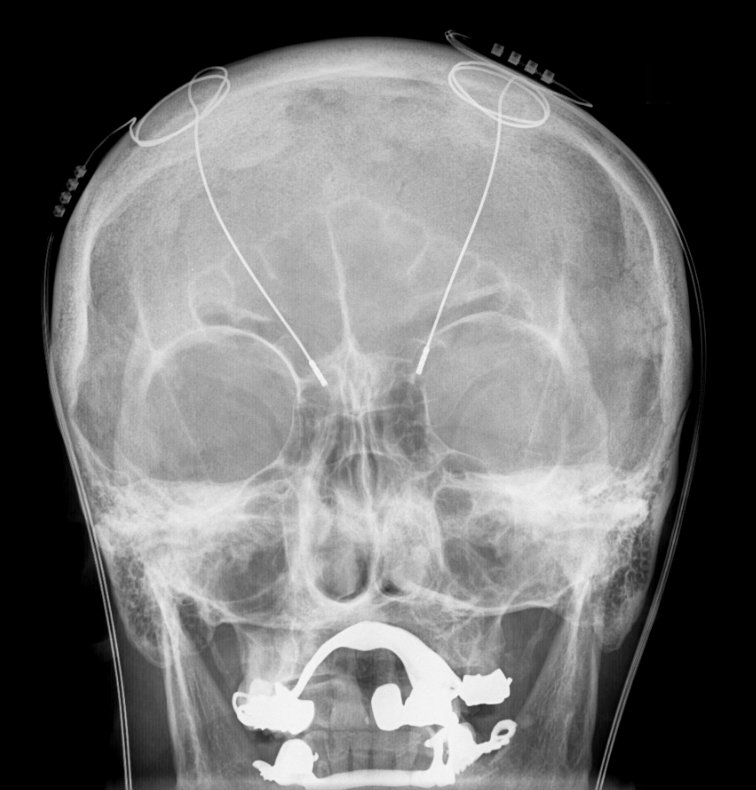
Deep Brain Stimulation (DBS) is a major neurosurgical procedure that’s indicated when medications do not control severe motor symptoms of Parkinson’s Disease. Prior to surgery, image studies are obtained to pin-point the targeted area of the brain, such as the subthalamic nucleus thought to be implicated in PD.
The procedure is initially done while the person is awake and involves placing electrode(s) in the targeted area of the brain. Later under general anesthesia. the electrode is connected to a wire that runs from the head, down the neck and shoulder into the chest region where it is attached to a device called a pulse generator. Some have called this, a “brain pacemaker.”
Once the generator is turned on, it emits electrical signals twenty fours per day that change the brain’s neural activity. In people with PD, the objective is to block the brain’s activity that causes tremors and unwanted movements. As with all surgical procedures, there are risks involved and the procedure doesn’t work for everyone.
No one knows for certain what causes Parkinson’s disease. Nevertheless, genetics, exposure to toxins, head trauma and certain antipsychotic and other medications have been associated with PD. What is known is that the loss of dopamine over time, brings on the symptoms of PD. Treatment manages the symptoms of PD, but it doesn’t change the progressive, or the debilitating course of the disease.
What can you do? It useful to join an exercise program and participate in a support group. Become an expert at understanding the medications you are taking and their side effects. Take note, as your dopamine levels fluctuate, so might your behavior. Avoid becoming isolated and some suggest don’t hide the fact that you have Parkinson’s disease. Look for neurologists with special training in movement disorders
Currently, there are several treatment options, and ongoing research with many clinical trials aimed at curing this disease. The Parkinson’s Foundation, and the Michael J. Fox Foundation for Parkinson’s Research are two sources to get information about clinical trials.
References
- National Institute of Neurological Disorders and Stroke; Parkinson’s Disease Information Page; 2019
- National Institute of Neurological Disorders and Stroke; Parkinson’s Disease: Hope Through Research; 2019
- Parkinson Foundation: What is Parkinson’s Disease?
- Michael J. Fox Foundation; Resources for People Newly Diagnosed with Parkinson’s
- Oleh Hornykiewicz; A Brief History of Levodopa; J Neurol, Nov 2010
- Joseph R. Anticaglia, MD; An Overview of Parkinson Disease; Doctor’s Column, HC Smart, 2020
- Joseph R. Anticaglia, MD; Non-Movement (Non-Motor) Symptoms of Parkinson’s Disease; Doctor’s Column, HC Smart, 2020
- Joseph R. Anticaglia, MD; Early and Late Stages of Parkinson’s Disease — Five Stages of PD; Doctor’s Column, HC Smart, 2021
Glossary
COMT — Catechol-O-methyltransferase, e. g., Encapapone
Addendum
Lewy body dementia (LBD) is the second most common type of progressive dementia after Alzheimer’s disease. This disease is associated with abnormal deposits of a protein in the brain called alpha-synuclein. When these abnormal protein deposits clump-up, they are called Lewy bodies which researchers theorize can lead to problems with movement, thinking. emotions, and behavior.
This article is intended solely as a learning experience. Please consult your physician for diagnostic and treatment options.